
Commentary · Aesthetic Intelligence · Vol 1 · Issue 4
The Dunning–Kruger Curve in Aesthetic TrainingWhy Injectors Are Blind to the Dip
A one-weekend certificate launches an injector at the top of Mt. Stupid — and what surgery does, with selection and mentorship, aesthetics still does not.
HSI Team1
- 1 Harley Street Institute, London, United Kingdom
Corresponding author: journal@harleystreetinstitute.com
Journal: Aesthet Intell
DOI: to be assigned
Volume / Issue: 1 / 4
Pages: 67–82
Received: 2025-09-10
Accepted: 2025-10-30
Published: 2026-05-30
Licence: CC BY 4.0
From the Editor's Desk
There is a particular look that comes over a face after one weekend of injectables training. It is the look of someone who has just been handed the keys to a Ferrari and assured, by a man with a stand at an exhibition, that the brakes are intuitive. They walk out of the room not knowing what they don't know — and, more importantly, not knowing that this is itself a known clinical state, named after two psychologists from Cornell, and reproducible in any field where the feedback loop is slow and the mirrors are flattering.
Aesthetic medicine is almost laboratory-designed for the dip. The patient pays cash, smiles in the mirror, and posts a photograph. The injector mistakes applause for evidence. By the time the granuloma, the migration, the asymmetry or — at the unlucky end of the curve — the vascular event arrives, the operator has accumulated three years of confidence and very little of the chastening that real medicine usually supplies. This essay is about the dip nobody falls into, and why the absence of the fall is the most dangerous thing about it.
Abstract
- Background.
- The Dunning–Kruger effect describes a robust cognitive bias whereby individuals with limited competence in a domain systematically overestimate their ability, while genuine experts tend to underestimate theirs (Kruger & Dunning, 1999). In non-surgical aesthetic medicine — where short foundation courses are commercially abundant, regulation is fragmented, and the consequences of error include blindness and skin necrosis — this bias appears to operate with unusual force.
- Methods.
- Narrative commentary synthesising the original Dunning–Kruger literature, subsequent replications and critiques, the medical-education evidence on self-assessment accuracy, and contemporary safety data from the aesthetic-injectables literature. An informal reader survey is embedded to allow practitioners to map their own pre-course and post-course confidence onto the canonical curve.
- Results.
- Three structural features distinguish aesthetic training from surgical training and amplify the early confidence peak: (i) extreme compression of the learning timeline, often a single 1–2 day course before independent practice; (ii) deferred and statistically rare feedback, since severe vascular complications occur in the order of 0.001–0.05% per mL injected; and (iii) immediate social and financial reinforcement from cosmetic outcomes that look successful in the first 48 hours regardless of injection plane. Surgical pathways, by contrast, are designed around prolonged supervised exposure that forces practitioners through the Valley of Despair before independent operating.
- Conclusion.
- Extensive, longitudinal, supervised aesthetic training is not a marketing claim — it is the structural mechanism by which a practitioner is moved past the Dunning–Kruger peak into calibrated competence. Courses that end at the peak, by design or by default, leave the public exposed.
Keywords: Dunning–Kruger effect, metacognition, self-assessment, aesthetic training, injectable safety, deliberate practice, medical education
Postgraduate Level
Equivalence to 1 CPD/CME point — we do not award CPD/CME directly
Read the article, complete a short assessment, and submit your reflection to receive your AiCE Points certificate.
Take Assessment & Get CertificateLearning Objectives
- •Recognising the metacognitive basis of the Dunning–Kruger effect in clinical skill acquisition
- •Understanding why aesthetic training architecture amplifies the early confidence peak
- •Designing supervised pathways that deliberately produce the Valley of Despair before independent practice
- •Using personal case logs, peer review and complication drills as calibration tools
Dunning–Kruger Self-Audit
Where Am I on the Curve?
- Mt. Stupid
- <50 supervised cases
- Valley
- First serious complication
- Slope
- Mentored case logging
- Plateau
- >5 yrs + peer review
Structural Correctives
- Selection
- Entry standards beyond a deposit
- Mentorship
- A named senior, not a WhatsApp group
- Logbook
- Every case, every outcome, every revision
- Audit
- Quarterly outcome review, not just CPD hours
Share this article
Download the card below or share the article directly. Tag @harleystreetinstitute.
Commentary · Aesthetic Intelligence
Why aesthetic injectors are blind to the Dunning–Kruger dip.
A one-weekend course launches a practitioner at the top of the confidence curve — and rarely forces them through the valley.
- EffectBottom-quartile performers self-rate in the top third (Kruger & Dunning, 1999).
- Vascular event rate~1 per 6,410 injections per syringe (Alam et al., 2021).
- Surgical contrastSelection, supervised rotations, named mentorship — all standard, all absent in most aesthetic training.
- Feedback delayCosmetic outcomes look successful in the first 48 h regardless of injection plane.
- ImplicationExtensive longitudinal training is the structural mechanism, not a marketing claim.
Aesthetic Intelligence
The Harley Street Institute
harleystreetinstitute.com
1. Introduction
In 1999, the social psychologists Justin Kruger and David Dunning published a now-iconic paper in the Journal of Personality and Social Psychology titled "Unskilled and Unaware of It" (Kruger & Dunning, 1999). Across four studies in domains as different as humour, logical reasoning and English grammar, they demonstrated that participants in the bottom quartile of actual performance estimated themselves, on average, to be in the top third. The effect was not stupidity: it was a metacognitive failure. The very skills required to perform competently in a domain are the same skills required to recognise incompetence in oneself. People at the bottom of a competence distribution are therefore doubly cursed — they perform poorly, and they cannot see that they perform poorly.
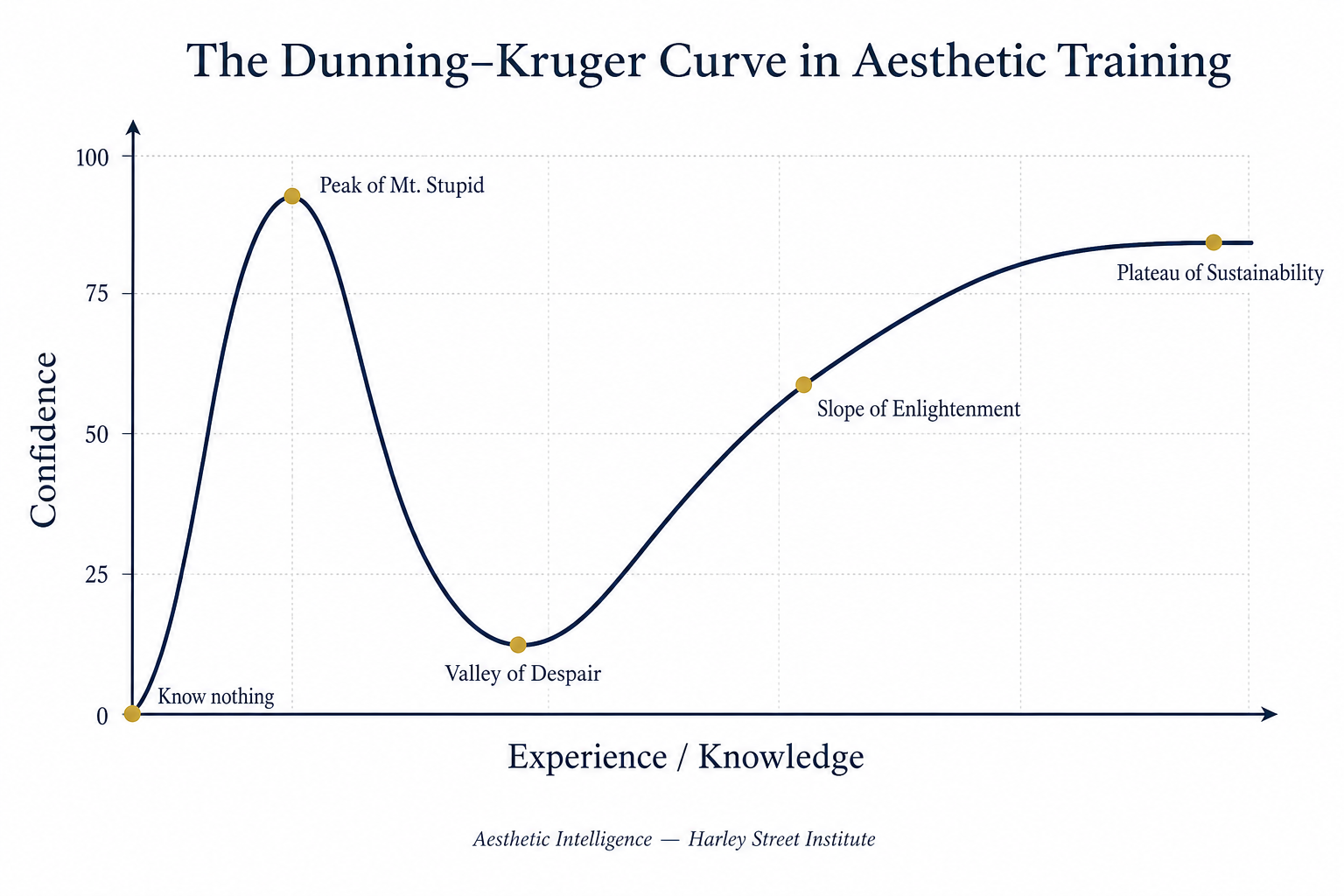
The popular caricature of the curve — the so-called "Peak of Mt. Stupid" followed by the "Valley of Despair", the "Slope of Enlightenment" and the "Plateau of Sustainability" — is, strictly speaking, an internet meme rather than a figure from the original paper. But it is a meme that has survived because it captures something real about how people experience the acquisition of a high-stakes skill (Dunning, 2011). In medicine, and especially in non-surgical aesthetic medicine, that curve is not merely amusing. It is a patient-safety problem.
This commentary makes a specific claim. Aesthetic practitioners are not biologically more susceptible to the Dunning–Kruger effect than other clinicians. They are, however, placed in a training and market environment that is almost perfectly engineered to keep them on the early peak — and to obscure the dip that, in surgery, is forced upon every trainee whether they want it or not. Understanding why is the first step to designing training that crosses the valley rather than stopping at the summit.
2. What Dunning and Kruger Actually Showed
Kruger and Dunning's original study used four converging experiments. Cornell undergraduates were assessed on humour judgement (using jokes pre-rated by professional comedians), formal logical reasoning, and grammar. Across all domains, participants in the lowest quartile of actual performance produced wildly inflated self-rankings; participants in the highest quartile produced slightly deflated ones (Kruger & Dunning, 1999, pp. 1121–1125). Crucially, when low-performing participants were subsequently trained in the relevant skill, their self-assessment accuracy improved — not because their estimates of themselves changed dramatically, but because they could now recognise quality in others.
Subsequent work has refined, contested and, importantly, replicated the core finding. Ehrlinger and colleagues (2008) demonstrated that the effect persists even when participants are offered monetary incentives for accurate self-assessment, ruling out a simple impression-management explanation. Critics such as Nuhfer and colleagues have argued that part of the visual pattern is a statistical artefact of regression to the mean, but the substantive metacognitive gap — that those who know least cannot reliably know how little they know — remains intact across multiple methodologies (Dunning, 2011).
The clinically important translation is this: subjective confidence is a poor proxy for competence at the lower end of the skill distribution, and this is the very end of the distribution that a freshly-certified injector occupies on day one of independent practice.
3. Why Medicine — and Aesthetic Medicine Especially — Is Vulnerable
A 2006 systematic review in JAMA examined 17 studies comparing physicians' self-assessment with externally observed measures of competence (Davis et al., 2006). The review concluded that physicians' ability to self-assess is, in general, poor, and that the least skilled clinicians were the most likely to overestimate themselves — a domain-specific replication of Dunning and Kruger inside medicine. The authors explicitly warned against relying on physician self-assessment as a primary mechanism of continuing professional development.
Aesthetic medicine concentrates and amplifies the conditions Davis described, for three structural reasons.
First, the training timeline is compressed to an extent that has no parallel in surgical specialty training. A practitioner can, in many jurisdictions, complete a one- or two-day foundation course in botulinum toxin and dermal filler and begin treating private patients the following Monday. Surgical training, by deliberate design, runs for years, with supervised case logs, structured assessments and graded responsibility. The Dunning–Kruger peak in surgery is something a trainee is dragged through under supervision. In aesthetics it is, too often, the launch pad for independent practice.
Second, the feedback loop is rare and delayed. The serious complications that should, in principle, calibrate an injector's confidence are statistically uncommon. Vascular occlusion is reported at an incidence in the order of 0.001–0.05% per millilitre of filler injected (DeLorenzi, 2014), and visual loss from dermal fillers, while devastating, is a rare published event with fewer than 200 fully-documented cases worldwide at the time of the 2015 Beleznay review (Beleznay et al., 2015). A new injector can therefore complete dozens — sometimes hundreds — of treatments without ever encountering an adverse event severe enough to disturb the early confidence peak. The absence of disaster is mistakenly read as evidence of skill.
Third, the cosmetic feedback signal is almost entirely positive in the first 48 hours. A lip filler placed in the wrong plane still looks plump on the day of treatment. A toxin dose placed in the wrong muscle still produces movement reduction. The patient leaves happy, posts a photograph, refers a friend. By the time a delayed nodule, vascular event or asymmetry emerges, the practitioner has already received multiple iterations of social and financial reinforcement that read, internally, as competence.
4. Why Surgery Forces the Dip — and Aesthetics Often Does Not
Surgical training is, in metacognitive terms, a structured machine for producing the Valley of Despair. A foundation-year doctor scrubs in, holds the camera, retracts, closes — and is reminded, every day, of what they cannot yet do. They are not permitted to operate independently until they have observed, assisted and been observed across a defined volume of cases. By the time independent operating begins, the surgical trainee has accumulated enough exposure to specific complications to have a calibrated, often anxious, internal model of risk.
There is a second filter that operates in surgery long before the trainee ever holds a scalpel: selection. Entry into a surgical training programme is competitive, examined and externally adjudicated. A consultant or programme director signs off on suitability. A national selection process screens for technical aptitude, judgement and temperament. Local rotations distribute trainees to firms where a named senior is professionally accountable for their development. And, critically, every surgical trainee operates inside a long mentorship relationship — sometimes years with the same firm — in which an experienced surgeon's standing eye on the trainee is the principal calibration instrument. Aesthetic medicine, in most markets, has none of this. There is no selection committee for a weekend filler course. There is no local rotation. There is no named mentor with a professional reputation attached to your trajectory. The trainee enters, pays the fee, attends, and leaves certified. The filter that surgery applies before the Valley of Despair even becomes relevant is, in aesthetics, absent.
Anders Ericsson's work on deliberate practice underpins the design philosophy of supervised pathways (Ericsson, 2008). Expert performance, across surgery, music and chess alike, is the product not of unstructured experience but of long, supervised, error-corrected practice against a specific reference standard. The Valley of Despair is not a regrettable side-effect of surgical training; it is the active ingredient. It is the phase in which the trainee learns what they do not know, and acquires the metacognitive scaffolding required for safe independent practice. Selection, supervision and mentorship are the scaffolding that makes the descent into the Valley survivable.
Aesthetic training pathways, as currently structured in most markets, frequently omit all three. A one-weekend course, an online module and a certificate produce a practitioner who has never been selected against an external standard, never been observed under load by a named mentor, and never been forced — by case volume or by an examiner — to confront the boundaries of their competence. The result is a confident, certified, and metacognitively miscalibrated injector. This is not a moral failing of the practitioner. It is a predictable output of the training architecture.
5. The Specific Question: Why Are Aesthetic Practitioners More Blind?
There is no published evidence that aesthetic practitioners are constitutionally more susceptible to the Dunning–Kruger effect than other clinicians. What the surrounding literature and market structure suggest is that they are systematically denied the inputs that would normally correct it. Five interacting factors appear to matter.
(i) Commercial incentives favour brevity. Course providers compete on the speed at which a delegate can be certified to practise. A two-day course sells better than a two-year fellowship. The commercial pressure pushes training in the opposite direction to calibration.
(ii) Regulation is fragmented. In the United Kingdom, until very recently, there was no statutory requirement for cosmetic injectors to hold medical qualifications, and registration with bodies such as the Joint Council for Cosmetic Practitioners (JCCP, 2018) remained voluntary. Where regulation does not enforce supervised practice volumes, market behaviour fills the vacuum, and the market rewards confidence, not calibration.
(iii) Social media operates as a confidence amplifier. Before-and-after photographs, taken at the moment the patient leaves the chair, reach thousands of viewers and other practitioners. Slow-developing complications, when they occur, are rarely posted by the same accounts. The visible distribution of outcomes is selection-biased toward apparent success.
(iv) Cosmetic outcomes are subjective. Unlike a tibial fracture reduction, which is either anatomically aligned on a radiograph or it is not, a lip filler outcome can be defended as "the look the patient wanted". This grants the practitioner a soft escape route from objective feedback at exactly the points where calibration would otherwise occur.
(v) Severe complications are statistically rare per practitioner-year but devastating per event. A practitioner can spend years on the early peak before encountering an event that would force them into the Valley of Despair. The longer the peak lasts, the more confident — and the more independent — the practitioner becomes before any genuine recalibration occurs.
6. The Role of Extensive Training: Engineering the Valley on Purpose
If the early confidence peak is a structural product of short, unsupervised training, then the corrective intervention is structurally extended, supervised training. This is the core argument for fellowship-length aesthetic pathways. A 6- to 12-month supervised programme that combines live-model injecting, OSCE-style assessment, structured complication drills and faculty observation does not simply add hours to a foundation course. It changes the metacognitive trajectory.
Three mechanisms appear to be active. First, repeated supervised exposure produces enough varied case volume to encounter the moderate-severity events — lumps, asymmetries, vascular blanching — that almost never appear in a one-weekend course but happen routinely across a year of real practice. Second, observation by an experienced faculty member produces external feedback that the practitioner cannot generate internally, directly addressing the metacognitive blind spot identified by Kruger and Dunning. Third, structured complication scenarios — hyaluronidase escalation drills, vascular emergency walkthroughs, written and OSCE-format assessment — manufacture, in a controlled environment, the Valley of Despair that the market would otherwise allow the practitioner to avoid until a real patient pays the price.
Kirkpatrick's four-level model of training evaluation (Kirkpatrick & Kirkpatrick, 2006) is useful here. Most aesthetic courses measure only Level 1 (delegate reaction) and Level 2 (knowledge acquisition). A fellowship-style programme is designed to evaluate Level 3 (behaviour in independent practice) and Level 4 (clinical outcomes). It is at Levels 3 and 4 that Dunning–Kruger calibration actually occurs, because it is at those levels that the practitioner's behaviour is observed against an external standard rather than reported by the practitioner themselves.
7. Implications for the Aesthetic Practitioner
The practical reading of the literature is not that new injectors should not begin practising — it is that they should treat their post-foundation confidence with active suspicion, and structure the first 12–24 months of practice to engineer the Valley themselves. Practical correctives include: maintaining a logged case series with photographic follow-up at 1, 4 and 12 weeks rather than only at day-zero; presenting cases — including unflattering ones — to a peer group for external review; rehearsing hyaluronidase and vascular emergency protocols in scenario form before the event, not after it; and, above all, choosing post-foundation supervision over standalone courses.
The reader survey embedded with this article is designed as a small reflective tool. It is not a validated psychometric instrument. Its purpose is simply to make the gap between pre-course and post-course self-rated confidence visible to the reader, and — for those who have already encountered a real complication — to make the secondary drop visible as well. If your post-course self-rating jumped by 30 points or more, and your post-complication rating has not yet been tested, the most honest reading of the curve is that you have not yet entered the Valley.
That is not an indictment. It is an invitation.
Reader survey
Where are you on the curve?
Anonymous, stored only in your browser. Rate your self-perceived competence as an injector on a 0–100 scale at two points in time. Results are aggregated locally so you can compare your answers to other readers of this article on the same device.
This is a reflective tool, not a validated psychometric instrument. Responses never leave your device.
8. Conclusion
The Dunning–Kruger effect is not an insult and it is not a diagnosis. It is a well-replicated description of how human metacognition behaves in any high-stakes skill domain, and it operates on aesthetic practitioners with the same neutrality with which it operates on first-year surgeons, first-year pilots and first-year investors. What distinguishes aesthetic medicine is the absence of the institutional scaffolding — long supervised exposure, mandatory case logs, external assessment, mandatory complication drills — that other high-stakes professions use to drag their trainees through the Valley of Despair before independent practice begins.
The case for extensive, longitudinal, supervised aesthetic training is therefore not an argument from prestige. It is an argument from metacognition. It is the difference between a practitioner who has been certified at the Peak of Mt. Stupid and a practitioner who has been deliberately walked through the Valley, up the Slope of Enlightenment, and onto the Plateau where their confidence is, finally, an accurate signal of their competence. The public will not be able to tell the difference at the consultation. The complication, when it comes, will.
AI Disclosure
AI tools were used to assist with literature triage and copy-editing. All clinical claims, citations and conclusions were verified by the named author against primary sources. The figure illustrating the canonical Dunning–Kruger confidence curve was generated using a text-to-image model and is presented for didactic purposes only; it does not depict empirical data.
Competing Interests
The author(s) declare no competing financial or non-financial interests relevant to this work.
Funding
This work received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics & Consent
Where applicable, ethical approval and informed patient consent were obtained in accordance with the Declaration of Helsinki. Reviews and commentaries did not require ethical approval.
HSI Editorial · Reflection & Forward Recommendations
Where we stand on this
Reflection
The Dunning–Kruger effect is not a slur against new injectors. It is a structural prediction: anyone who completes a short, well-marketed course will overestimate their competence, because the metacognitive skill required to spot the gap is the same skill they have not yet developed. Surgery has known this for a century and built its training around it — selection, supervised rotations, named mentors, logbook-audited cases, a culture in which the trainee expects to be told they are wrong.
Aesthetics has built almost the opposite: open enrolment, a one-weekend certificate, no compulsory follow-up, no audit of outcomes, and a commercial incentive to sell the new injector a starter kit on the way out of the room. The peak of the curve is not an accident of personality; it is a product of the training architecture.
Forward Recommendations
- Reframe certification as the start of supervision, not the end of training. A practitioner who has completed a foundation course should be in mentored practice for a defined period before independent injecting is signed off.
- Mandate a personal case log with photographs and revision-rate audit. The single fastest way through the Valley of Despair is being shown your own week-12 outcomes alongside a senior's.
- Adopt selection criteria at training entry — clinical background, motivation, complication-management baseline — rather than treating every applicant as commercially equivalent. Aesthetics should be at least as selective as a surgical fellowship.
- Forward research direction: prospective cohort data correlating training architecture (duration, supervision intensity, audit frequency) with complication rates and patient-reported outcomes. The field cannot improve what it does not measure.
Editorial position of the Harley Street Institute. Authored by the HSI Clinical Review Board; not a substitute for the peer-reviewed evidence summarised above.
References
- Kruger J, Dunning D. Unskilled and unaware of it: how difficulties in recognizing one's own incompetence lead to inflated self-assessments. J Pers Soc Psychol. 1999;77(6):1121–1134.
- Dunning D. The Dunning–Kruger effect: on being ignorant of one's own ignorance. Adv Exp Soc Psychol. 2011;44:247–296.
- Ehrlinger J, Johnson K, Banner M, Dunning D, Kruger J. Why the unskilled are unaware: further explorations of (absent) self-insight among the incompetent. Organ Behav Hum Decis Process. 2008;105(1):98–121.
- Davis DA, Mazmanian PE, Fordis M, Van Harrison R, Thorpe KE, Perrier L. Accuracy of physician self-assessment compared with observed measures of competence: a systematic review. JAMA. 2006;296(9):1094–1102.
- Ericsson KA. Deliberate practice and acquisition of expert performance: a general overview. Acad Emerg Med. 2008;15(11):988–994.
- DeLorenzi C. Complications of injectable fillers, part 2: vascular complications. Aesthet Surg J. 2014;34(4):584–600.
- Beleznay K, Carruthers JD, Humphrey S, Jones D. Avoiding and treating blindness from fillers: a review of the world literature. Dermatol Surg. 2015;41(10):1097–1117.
- Goodman GJ, Magnusson MR, Callan P, et al. A consensus on minimizing the risk of hyaluronic acid embolic visual loss. Dermatol Surg. 2020;46(12):1531–1538.
- Joint Council for Cosmetic Practitioners (JCCP). Competency framework for cosmetic practitioners. London: JCCP; 2018.
- Kirkpatrick DL, Kirkpatrick JD. Evaluating training programs: the four levels. 3rd ed. San Francisco: Berrett-Koehler; 2006.
© 2026 Harley Street Institute. Published under the Creative Commons Attribution 4.0 International Licence (CC BY 4.0).
Post-publication review
Discuss this article with the journal AI
Ask a clinical question about this article, or flag a possible error. Our AI agent will reply in real time, log your input, and — if you have identified a credible mistake — escalate it to the HSI editorial team for review and a published correction notice.
AI responses are generated by an assistant model. They do not constitute medical advice. Editorial corrections are only applied after a named HSI editor reviews and signs off.
Hi. I'm the Aesthetic Intelligence reader AI for this article.
Try: "Explain section 3 in plain English." · "What's the evidence for the 1-in-6,410 figure?" · "How does this compare to UK NICE guidance?"