
Introduction to Infective & Reactive Dermatoses
Why barrier disruption defines aesthetic risk
Let's be honest about what we do for a living. Aesthetic medicine is the polite art of injuring people on purpose. Microneedling punches holes through the epidermis. Peels dissolve the stratum corneum. Lasers cook the dermis. Injectables skip the foreplay entirely and go straight through it. We call it rejuvenation because "elective, paid-for trauma" doesn't sit well on a consent form — but the biology doesn't care what we call it. Every result we sell is a wound-healing response we triggered, and every wound is, by definition, an open invitation.
Most patients RSVP politely. A few don't. The folliculitis after microneedling, the cold sore blooming five days after a perioral peel, the erythema that overstays its welcome for three weeks — none of this is exotic. None of it is bad luck. It is what happens when you disturb a system that spent a few million years learning to keep microbes out and inflammation quiet, and then act surprised when it complains.
The thesis of this module is unromantic: prevention is cheaper, easier, and considerably less embarrassing than treatment. A proper history, clean technique, antivirals when the patient's lip has form, and aftercare instructions the patient might actually read — that alone removes most of the problems before they exist. Everything that gets through that net then becomes a recognition problem. The clinicians who get into trouble are rarely the ones who treated badly; they are the ones who looked at something unusual and decided it was probably nothing.
This module covers the full menu — bacterial, viral and fungal infections, HSV reactivation, contact dermatitis, urticaria, and the procedural complications that tie them together. The mindset is the one you've been building all the way through this programme: risk-layered, slightly paranoid, and quietly aware that the cost of missing a complication is always higher than the cost of looking foolish for being careful.
Clinical Takeaway
Every aesthetic procedure is a deliberate breach of the skin's defensive system. The clinician's task is to anticipate the consequences of that breach, not just deliver the technique.
Frequently Asked Questions
How common are infective complications in aesthetic medicine?
They are uncommon in well-run practices but never zero. Reported rates vary by procedure but folliculitis, HSV reactivation and contact dermatitis are the most frequent.
Are these complications avoidable?
The majority are. Robust pre-procedure assessment, aseptic technique, prophylaxis where indicated, and patient education prevent most events before they begin.
Key Points
- Aesthetic procedures rely on controlled injury — which inherently elevates infection risk
- Complications are uncommon but predictable, not exotic
- Prevention through technique and screening outperforms treatment
- Early recognition is the second line of defence
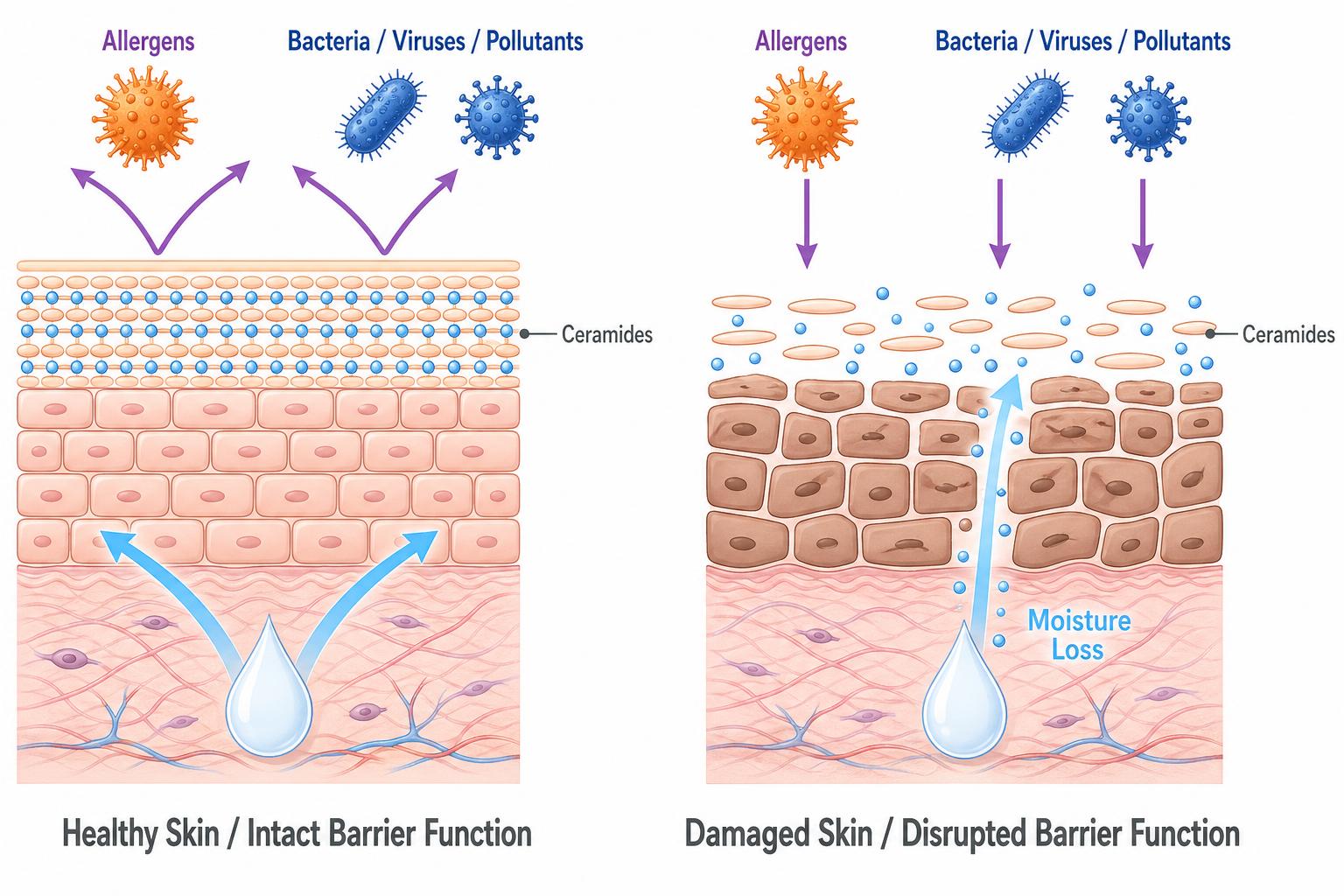
- The risk profile of every procedure is shaped by barrier disruption
Clinical Tip
Before every procedure, ask yourself one question: "If this patient develops a complication, what will I see first, and what will I do?" If you cannot answer instantly, you are not yet ready to treat.
Continue Your Clinical Dermatology Training
This page is part of the CAD – Certificate in Aesthetic Dermatology by Harley Street Institute. Unlock the full structured programme to build clinical confidence in dermatological assessment.