
Barrier Function in Practice
Recognising and managing barrier dysfunction
In clinical practice, barrier function is a key determinant of how the skin responds to any aesthetic intervention. At a histological level, the barrier is primarily located within the stratum corneum, where corneocytes are embedded in a lipid matrix composed of ceramides, cholesterol, and free fatty acids. This "brick and mortar" structure regulates transepidermal water loss (TEWL) and protects against external irritants.
When the barrier is compromised, there is disruption of this lipid matrix, leading to increased TEWL and reduced cohesion between corneocytes. This results in microfissuring of the skin surface, allowing irritants, allergens, and microorganisms to penetrate more easily. At the same time, keratinocyte signalling pathways become activated, releasing pro-inflammatory cytokines that further amplify skin reactivity.
Clinically, this presents as dryness, flaking, erythema, and heightened sensitivity. Patients often report stinging or burning even with mild products. Importantly, this state reflects not just surface dryness, but an underlying inflammatory and structural imbalance.
Performing aesthetic treatments on compromised skin can exacerbate this cycle by further disrupting the barrier and prolonging inflammation. Instead, the priority should be to restore lipid balance, reduce inflammation, and allow normal epidermal turnover to resume.
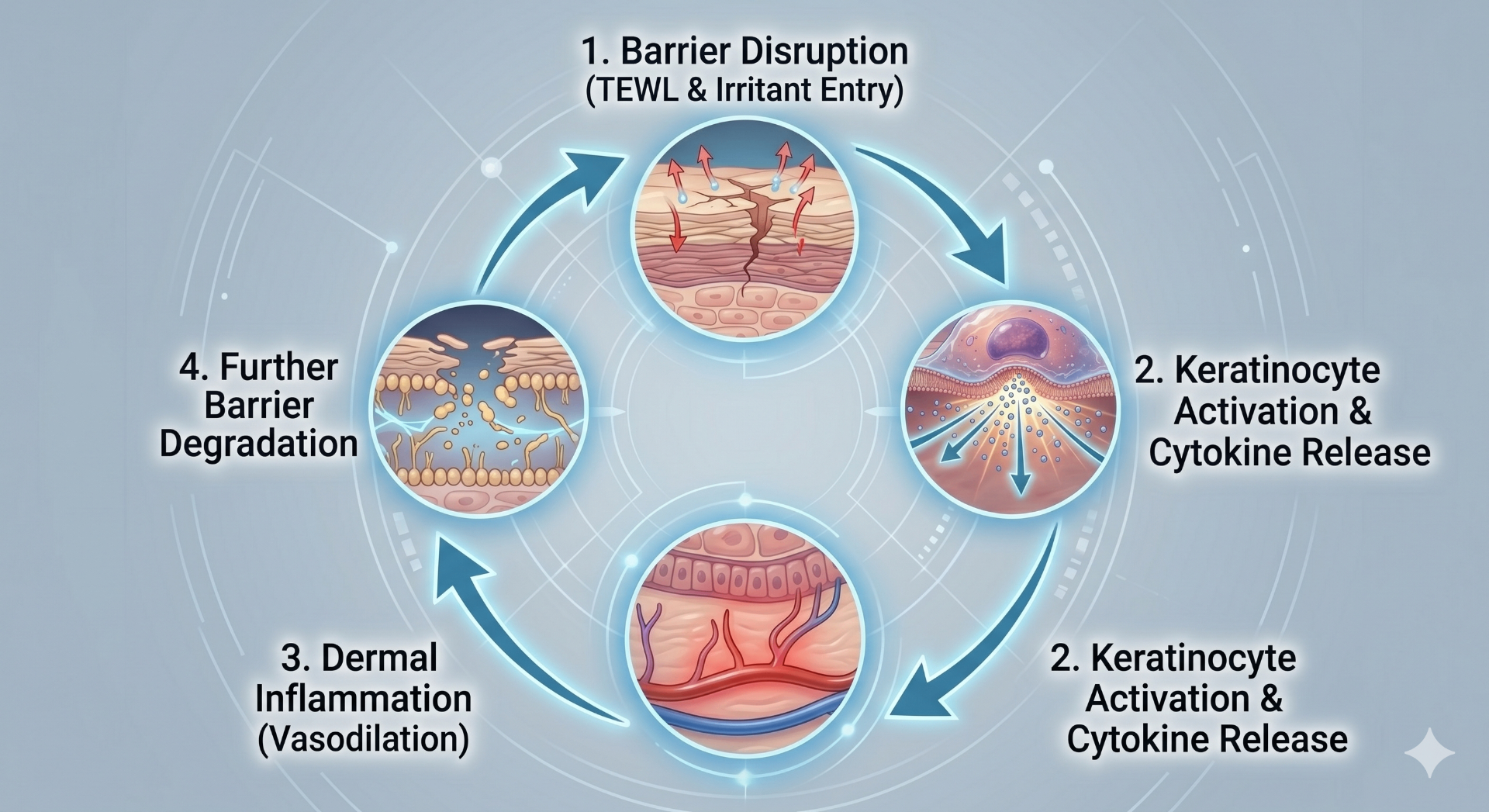
To visualise this key feedback loop, consider the circular, multi-stage process: starting at 1. Barrier Disruption (TEWL and irritants enter), which then triggers 2. Keratinocyte Activation and Cytokine Release, leading to 3. Dermal Inflammation (Vasodilation), and completing the loop with 4. Further Barrier Degradation. This self-perpetuating cycle is why early intervention and barrier repair are critical.
Treating the barrier first not only improves safety but also enhances the effectiveness and predictability of future treatments.
Clinical Takeaway
Barrier dysfunction is not just surface dryness — it is a structural and inflammatory disruption of the epidermis. Stabilise the skin first, then treat.
Frequently Asked Questions
How do I recognise barrier dysfunction?
Barrier dysfunction presents with dryness, flaking, increased transepidermal water loss, and heightened sensitivity. Patients often report stinging or burning with products that were previously tolerated. Histologically, this reflects disruption of the lipid matrix and increased inflammatory signalling within the epidermis.
Should I treat patients with compromised barriers?
No. Performing aesthetic procedures on compromised skin can worsen inflammation, increase TEWL, and lead to complications such as post-inflammatory hyperpigmentation. Management should focus on barrier repair, reduction of irritants, and restoration of epidermal homeostasis before any intervention.
Key Points
- Barrier function depends on an intact stratum corneum and lipid matrix
- Disruption leads to increased TEWL and inflammatory signalling
- Clinical signs include dryness, flaking, erythema, and reactivity
- Treating compromised skin can worsen outcomes
- Barrier repair must precede aesthetic intervention
Continue Your Clinical Dermatology Training
This page is part of the CAD – Certificate in Aesthetic Dermatology by Harley Street Institute. Unlock the full structured programme to build clinical confidence in dermatological assessment.